FieldStrength MRI magazine
Educational - August 2016
UMC Utrecht offers insight in their experiences with integrating MRI into radiation therapy planning workflows
Radiation therapy (RT) uses imaging to support delineating anatomy for dose planning. In general, the aim is to target the tumor and spare the surrounding tissues as much as possible. This requires careful planning to ensure spatial accuracy and calibrated dosing. University Medical Center Utrecht (Utrecht, Netherlands) has embraced MRI to enhance radiation therapy planning with the benefit of its high soft tissue contrast.
“Using MRI in radiation therapy means we can differentiate soft tissues and visualize organs and anatomical structures”

Marielle Philippens, MD, PhD
Marielle Philippens, MD, PhD, has been a radiobiologist and medical physicist with focus on MRI physics in the department of Radiation Oncology at University Medical Center Utrecht since 2008. Her research interest is functional imaging for oncology, with particular focus on diffusion weighted MR imaging. Her research focus areas are head and neck cancer, rectal cancer and breast cancer.
Good delineation can help spare critical anatomical structures
Advances in radiation therapy delivery devices allow more complex dose plans to be made. This drives the need for better delineation of tumors and surrounding tissues, but defining the target volume is still a challenge. Target delineation allows the radiation dose to be tailored to the anatomy [1-4] so that a high dose can be directed to the tumor, and a lower dose to the surrounding tissue. Ultimately, less radiation on surrounding tissue may help to preserve functionality of healthy tissue.
While CT is used as the standard imaging modality, it suffers from limitations in providing good soft tissue contrast, especially in regions where soft tissue structures are in close proximity to each other [1]. In this context, the benefits of MRI for radiation therapy treatment planning are long recognized.
MRI offers high soft tissue contrast, thereby providing anatomical as well as functional information for organ delineation and visualization of surrounding anatomy and critical structures, thereby helping to support good determination of target volume [1] “In treatment of the head and neck, for instance, we always try to save the parotid glands and the salivary glands. In cases of prostate and cervix cancer, we aim to spare the bladder and rectum as much as possible. To achieve this, we need to first find the outline of the target. In my experience, it can be quite difficult to delineate this with CT, even when using contrast agent. This is why the high soft tissue contrast of MRI is attractive for radiation therapy planning.”
Marielle Philippens, MD, PhD, a medical physicist in the radiotherapy department at UMC Utrecht, further explains:
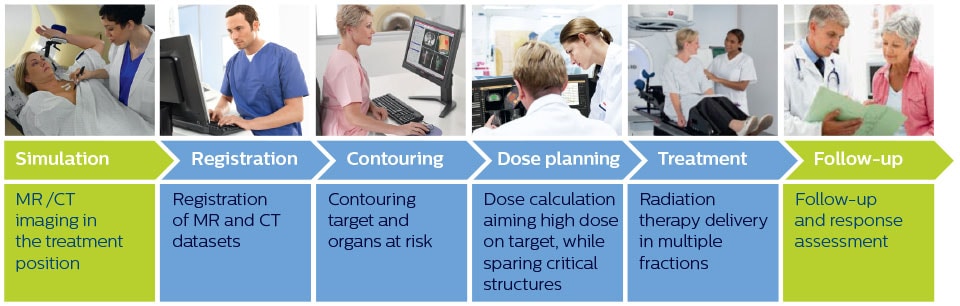
Simplified overview of MR imaging in radiation therapy workflow
Imaging plays a vital role at several steps in the radiation therapy workflow to visualize targets and critical structures for contouring, and to assess treatment response.
Choosing MRI protocols for treatment planning
In clinical practice, MRI is mostly used in conjunction with CT for visualization of targets and critical structures [5], while CT is used to delineate anatomical structures and provide Hounsfield Units (HU) for dose calculation.
“MRI can provide different types of contrast,” says Dr. Philippens. “This allows us to see more details than on CT. We can differentiate soft tissues and visualize organs and anatomical structures, but it takes some experience, particularly with head and neck tumors, to understand how to interpret the details seen in the image.”
“MRI can provide anatomical and functional information. The most important sequence for tumor delineation is the T1-weighted scan after contrast administration. On post-contrast T1-weighted MR images with fat suppression, the tumor can be distinguished due to its high perfusion and leaky vessels. We also use pre-contrast T1- weighted images, which show tumor extension into the fatty tissue.
“On the T2-weighted MRI with fat suppression the tumor with its edematous surrounding tissue can be clearly distinguished. This is particularly useful if the tumor does not show enhancement after contrast injection.
“Diffusion weighted imaging (DWI) shows very high contrast between the tumor and surrounding tissue. DWI helps us to see how a tumor extends into another structure, which we may not see on the T1-weighted or T2-weighted images. However, as DWI images are prone to distortions, these are mainly used to visualize the tumor and for response assessment, and not yet so much for delineation. I like to include diffusion weighted imaging, as it is so easy to see the tumor in these images. In my opinion, it has great potential, both for supporting tumor delineation and in response assessment.”
“I like to include diffusion weighted imaging, as it is so easy to see the tumor in these images. In my opinion, it has great potential for tumor delineation and response assessment”
")
")
Successful planning requires a good fit between MRI and CT
Ideally, the patient position during the MRI scan should be exactly the same as during radiation therapy treatment, to ensure that organs are in the same position and that the target volume planned on the images will match the volume that is irradiated. Therefore, a flat tabletop and an external laser for patient alignment are often used during MRI to obtain spatial correlation in radiation therapy treatment planning and good coregistration of MRI and CT images.
“For coregistration of MRI and CT images, we aim to use an MRI contrast type with few non-linearities and good tissue differentiation, preferably acquired as non-angulated axial slices,” says Dr. Philippens.
“Either 3D scan protocols or multislice 2D protocols with contiguous slices are used to allow target volume reconstruction in the different orthogonal directions.”
MRI is used for planning in a variety of anatomies
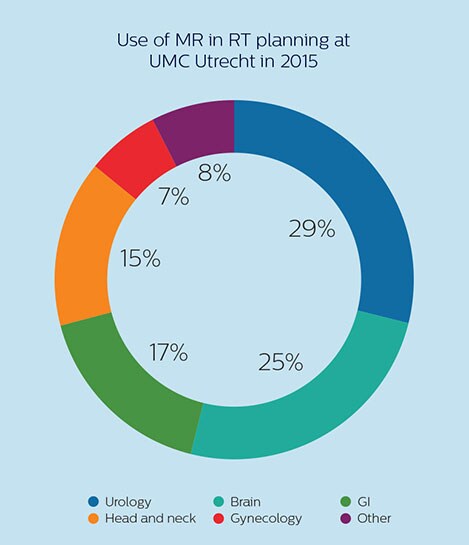
At UMC Utrecht, Dr. Philippens and her colleagues are using MRI in planning external beam radiation therapy (EBRT) for treatment of tumors in a variety of anatomies, such as organs in the pelvis (including bladder, prostate, rectum and cervix), the brain, the esophagus, pancreas, the larynx and oropharynx, bone metastases and sarcomas. In addition, MRI is also used to guide brachytherapy in the prostate and cervix. [6]
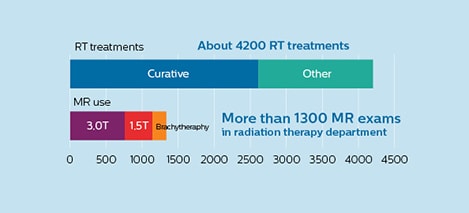
The University Medical Center Utrecht Department of Radiotherapy is a leading center in radiation therapy, continuously striving to improve methods and provide excellent patient care. UMC Utrecht has two Philips Ingenia MR-RT systems (1.5T and 3.0T) for RT treatment simulation as well as a Philips Ingenia 1.5T system dedicated for brachytherapy. Furthermore, it is an Atlantic MR-Linac consortium member.
“MRI also helps in visualizing the lesions inside the prostate, which may not be possible in CT.”
High dose on the lesion rather than on the whole prostate
MRI is capable of visualizing the prostate and the surrounding organs such as rectum, penile bulb, bladder, the apex and seminal vesicles, as well as visualizing intra-prostatic lesions [2,4].
“All our patients undergo an MRI exam – along with CT – before radiotherapy of the prostate,” says Dr. Philippens. “For prostate delineation, we are scanning a balanced TFE with fat suppression. We can also see the gold fiducial markers in these images, which are used for position verification and are therefore used for registration to CT. For geometric accuracy of the image, we choose a 3D sequence, which is corrected for the gradient non-linearities in all directions.
“In addition to helping in delineation of the prostate, MRI also helps in visualizing the lesions inside the prostate, which may not be possible in CT.
“When we can visualize intraprostatic lesions, the radiation therapist can then plan to boost them, giving a higher dose to those lesions instead of giving a uniform dose to the whole prostate, in the hope to better treat the patient and have less risk of recurrent tumors. However, this is not yet clinical routine. For visualizing the lesions, we not only use anatomical, T2-weighted imaging, but also diffusion weighted MRI and dynamic contrast- enhanced MRI."
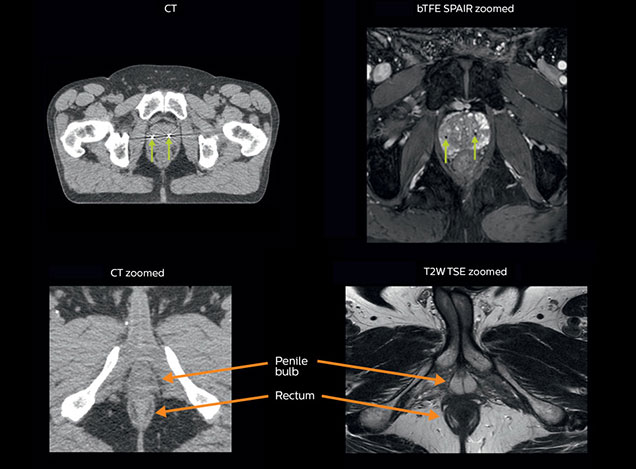
Visualizing critical structures with MRI before prostate radiation therapy
A 63-year-old patient with prostate cancer, cT3bNxM, Gleason 7, underwent MRI on Ingenia 3.0T MR-RT before radiation therapy.
Intraprostatic lesions are visible on the bTFE MR image, but not on the CT image. MRI shows excellent soft-tissue contrast for the visualization of critical structures like the rectum and penile bulb.
Fiducial markers (green arrows) are used in registration of MR images to CT, to transfer the MR-based delineations onto the CT image dataset.
“In patients with a primary tumor in the head and neck area, we use MRI in daily clinical RT practice to visualize the tumor and critical structures. This may be used to help sparing of critical structures.”
Visualizing critical structures in the head and neck
“In patients with a primary tumor in the head and neck area, we do use MRI in daily clinical radiation therapy practice to visualize the tumor and critical structures. This may be used to help sparing of critical structures, such as the parotid glands, submandibular glands, esophagus, optic nerves, brain stem and spinal cord [7]. And postoperatively we scan patients that have tumor growth along the cranial nerves for target delineation,” says Dr. Philippens.
“Because of the challenges posed by CT-MRI coregistration in this area with many degrees of freedom for motion, we image these patients in a radiotherapy mask. However, one disadvantage of using the mask is that a regular head and neck coil cannot be used; a dedicated coil solution would be needed for imaging with a mask.
For this we make use of flexible coils that we position close to the target area. This setup can also be combined with the anterior coil for a larger coverage and enhanced SNR.”
“We use pre- and post-contrast T1- and T2-weighted sequences with the fast and robust mDIXON method for fat suppression,” says Dr. Philippens. “Dynamic contrast-enhanced imaging is performed with high temporal resolution and low spatial resolution, to see the contrast agent uptake in the tumor. Diffusion weighted imaging is used qualitatively to see how the tumor extends into another structure, rather than for strict delineation.”
“In postoperative patients who have had tumor growth along the cranial nerves, we use T2-weighted gradient echo (FFE) on our 3.0T MR-RT scanner to show the nerves for target delineation and look to see if there is still tumor left.”
References
1. Schmidt MA, Payne GS. Radiotherapy planning using MRI. Phys Med Biol 2015, 60: R323–361 2. Doemer A, Chetty IJ, Glide-Hurst C, et al. Evaluating organ delineation, dose calculation and daily localization in an open-MRI simulation workflow for prostate cancer patients. Radiat Oncol. 2015;10:37. 3. Devic S. MRI simulation for radiotherapy treatment planning. Med Phys 2012, 39: 6701-11 4. Paulson ES, Erickson, B, Schultz C, Li XA. Comprehensive MRI simulation methodology using a dedicated MRI scanner in radiation oncology for external beam radiation treatment planning. Med Phys 2015, 42: 28-39
5. Glynne-Jones R, Nilsson PJ, Aschele C, et al. Anal cancer: ESMO-ESSO-ESTRO clinical practice guidelines. Ann Oncol. 2014;25:iii10-20. 6. Metcalfe P, Liney GP, Holloway L, et al. The potential for an enhanced role for MRI in radiation-therapy treatment planning. Technol Cancer Res Treat 2013, 12: 429-46 7. Nuyts S. Defining the target for radiotherapy of head and neck cancer. Cancer Imaging. 2007; 7:S50-5.
Results from case studies are not predictive of results in other cases. Results in other cases may vary.
Results from this facility are not predictive of results in other facilities. Results in other facilities may vary.